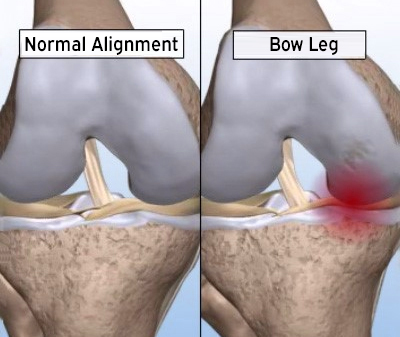
The knee joint can be divided into two halves, as inner and outer parts. While standing, body weight axis; starting from the head of the hip passing through the middle of the knee and the middle of the ankle. In this way, 60% of our body weight is reflected to internal knee and 40% to external knee parts. Thus, with age, the inner part of the knee wears earlier and the legs are bent inward. This is called ‘O Leg’ (crooked leg: genu varum).
Correction of Leg Curvature (High Tibia Osteotomy)
Because the inner part of the knee encounters more load on the leg leaning inward, the joint is worn out and calcified faster. Calcification and joint damage can accelerate the process that will lead the knee joint to knee replacement surgery.
Bone correction surgery that corrects this curvature is called ‘High Tibial Osteotomy (HTO)’. This is not a visual correction for aesthetic purposes; this is correction intervention in order to prevent early knee wear or delay prothesis surgery on the knees which only is worn at internal side.
Young patients with advanced leg curvature (distorted legs), although they request correction in the intention of aesthetic, it is necessary to perform leg correction with bone surgery at this age to maintain knee health.
Nowadays, 40- to 60-year-old patients with knee arthritis (worn cartilage of the inner knee cartilage) generally refer for HTO. The aim of the treatment in this age and injury group is gain 5-10 years to the patient before the knee prosthesis and to provide more painless and comfortable knee movements during this time.
The goal of OHR surgery; is to fix the leg curvature of the patient and to transfer the load from the worn cartilage region of the knee to the healthier outer side.
Whom can the YTO apply to?
- Applied in patients: Arthritis is on the inner side of the knee, when the outer side and kneecap is normal.
- There is no more than 25 degrees of curvature in the leg,
- In patients who are not overweight,
- There is not much movement limitation in the knee
- Without rheumatic knee stiffness.

What are the Benefits of YTO Surgery?
- Surgery is performed from under the knee. The natural joint structure is preserved because there is no intervention in the joint and no implant is inserted. Patients move more easily than the prosthesis.
- Delays knee replacement surgery for 5 to 10 years when performed to the appropriate patient group. The need for revision of the prosthesis, which may occur years after prothesis surgery, is reduced.
Operation method:
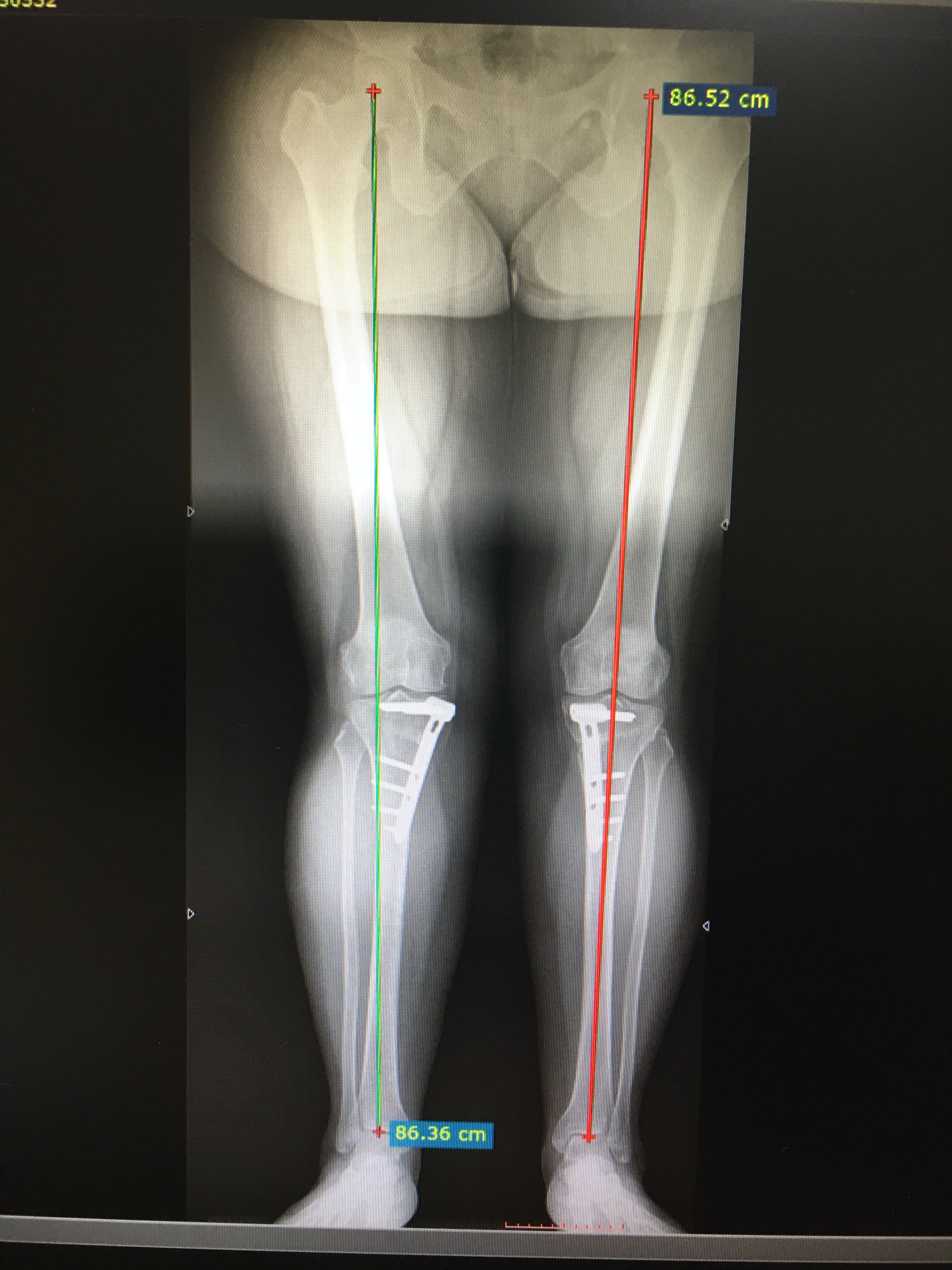
Pre-operative leg-length radiographs are taken to measure how much the leg load bearing axle shifted and how much the angulation is.
High tibial osteotomy is performed with open surgery. Before open surgery, arthroscopy (closed) method can be used to clear damaged cartilage inside the knee joint or to treat meniscus tears. By making bone incision under the knee in the surgery, when the desired angle is achieved, the bone is fixed with plate screws. Postoperative improvement of curvature of the leg can easily be seen. After high tibial osteotomy surgeries one or two nights stay in hospital is required, followed by walking with crutches for 6 to 8 weeks, then full load is allowed after 2 months.


What are the complications of surgery?
Although not seen as common, the main complications are can be line up as:
- vascular nerve damage during surgery
- swelling, pain, compartment syndrome
- infection
- clot formation in veins
- loosening breakage in plate screws
- not enough union of bone or complete non-union